Introduction
This guide synthesises the evidence on who to target, where to reach them, how to approach health behaviour promotion initiatives for young children, and what are the effective components of programs that can be tailored to specific contexts and environments.
Our previous research has highlighted the policy infrastructure and bold leadership needed for early childhood obesity prevention (read our evidence brief). This aligns with the overarching strategies outlined in the National Preventive Health Strategy and the National Obesity Strategy, which call for a systems approach that includes action from government, industry, the community and individuals. Our research to date has focused on settings and individual-level strategies that promote health behaviours to foster optimal growth.
Key Points
- Both universal and targeted approaches are needed to support obesity prevention in early childhood
- Promoting healthy growth and behaviours requires a multi-sector approach across different settings
- Various evidence-based strategies and approaches exist to promote health behaviours. Individual programs have limited impact without a broad range of actions across systems and settings to address the multiple drivers of obesity
- Healthy Beginnings and INFANT are scalable, evidence-based programs providing anticipatory guidance across multiple behaviours
Who to target? Both universal and targeted approaches are needed to encourage health behaviours in early childhood.

All young children can benefit from strategies that aim to promote healthy infant feeding, diet, enough physical activity and sleep, and that reduce screen time and sedentary behaviours. The latest ABS data show 94% of children (2-17 years) do not consume enough vegetables and 69% are not sufficiently active (AIHW).
Some children are at greater risk, including those from low socioeconomic backgrounds, Aboriginal and Torres Strait Islander, culturally and linguistically diverse and rural/remote communities. Universal programs are not currently meeting the needs of these priority groups. Prevention efforts should prioritise these groups to avoid exacerbating inequalities.
What are some different settings where programs promoting healthy growth can be implemented?
Promoting healthy growth and behaviours requires a multi-sector approach across different settings.
Primary health care
Primary health care is a key setting for prevention. In Australia, maternal child and family health nurses provide universal health and developmental checks from birth to school age – a key opportunity for health promotion during early childhood. Families have frequent contact with general practice throughout early childhood and beyond. GPs and practice nurses have an important role in promoting healthy growth, feeding, nutrition and movement behaviours during early childhood.
Strengthening prevention in primary care settings should be two-fold: building the capacity of the primary care workforce to confidently promote healthy growth and associated behaviours, and addressing systematic barriers to prevention including providing renumeration for preventive care.
Early childhood education and care (ECEC)
Nearly 50% of Australian children aged 0-5 years attend early childhood education and care, so this setting offers a significant opportunity to foster healthy behaviours in young children.
To maximise this potential, we need to build the ECEC sector’s capacity to advocate for, and integrate, health promotion practices into this setting. This includes establishing clear standards for healthy eating and physical activity and providing equitable support for implementation of these standards across ECEC services.
Child and family social/community services
Social and community services serve many vulnerable children who are at increased risk of suboptimal health behaviours and growth. Health promotion efforts in these settings should focus on equipping professionals with training to deliver brief interventions and providing tailored resources that address the specific needs of the families they serve.
Supported Playgroups have been highlighted as an opportunistic entry point to reach underserved families.
Evidence
Primary Health Care (PHC)
We reviewed Australian documents guiding PHC practitioners to support childhood growth, health, and development in the early years. While growth monitoring was widely recommended, guidance on screening and promoting health behaviours (diet, physical activity, sedentary behaviour, and sleep) was limited. Practical tools and comprehensive recommendations are needed for effective screening and health promotion in PHC. Integrating health behaviour screening tools into routine PHC could improve children’s health behaviours.
We undertook a systematic review evaluating child health behaviour screening tools in PHC settings including 22 studies on 14 tools. Results showed that health behaviour screening is acceptable and feasible for assessing children’s health behaviours in PHC, however, further research is needed to determine impact on child health outcomes.
In this commentary, we call for embedding health promotion and preventive care in Australian PHC to improve childhood health. We highlight challenges like time constraints and lack of training, while advocating for clearer guidelines, practical tools, and workforce development to strengthen health promotion and preventive care. Using the Ottawa Charter for Health Promotion, we propose actionable steps to create supportive environments, strengthen community actions, and develop necessary skills in PHC providers to improve child health outcomes.
This review explores improving access to primary health care and delivering healthy lifestyle advice in rural and regional areas of Australia for children in their first 2000 days. Findings suggest telemedicine, expanded nursing roles, and community health worker models can enhance care access. Further research on care models and partnerships is needed to prevent childhood obesity effectively.
This systematic review evaluated clinical practice guidelines (CPG) for preventing childhood obesity, focusing on the role of doctors. Eleven CPGs were reviewed, with seven considered high-quality. Key recommendations included growth monitoring, maintaining healthy weight, and promoting family involvement in healthy behaviours. The review highlighted a need for more practical and applicable guidelines to enhance implementation and impact.
This study explores current attitudes and perspectives for promoting child growth and health and preventing childhood obesity in Australian general practice. General practice staff agree on the importance of growth monitoring and promoting healthy behaviours, however barriers including systemic challenges and COVID-19 complications hinder routine implementation. Enablers include bridging the implementation gap and systemic changes to support these efforts.
Childhood obesity prevention in general practice: supporting implementation through co-ideation
Co-ideation workshops with Australian GPs and academics identified practical strategies for integrating childhood obesity prevention into general practice. Proposed interventions included GP education, clinical audits, accessible guidelines, resource repositories, and provision of adequate growth monitoring tools. These solutions address barriers and aim to support guideline implementation and preventive care activities to support children’s growth and health.
Primary healthcare professionals’ role in monitoring growth: a scoping review
Our scoping review of 36 studies exploring primary healthcare professionals’ practice in growth monitoring in high income countries found that, although most clinicians regularly weighed and measured infants, some lacked confidence in interpreting growth trajectories and discussing excessive weight gain with parents. Few interventions addressed unhealthy infant growth, highlighting the need for targeted training and support for primary care clinicians.
Early childhood education and care (ECEC)
There are no national Australian guidelines for ECEC food provision, and the comparability of existing jurisdictional guidelines is unclear. This project mapped and compared ECEC food provision guidelines and sought expert opinions on aligning them with the Australian Dietary Guidelines (ADG). Jurisdictional ECEC food provision guidelines were found to be inconsistent, raising challenges for national accreditation and the provision of support and resources for services across jurisdictions. Childhood nutrition experts supported national alignment of ECEC food provision guidelines. Implementing consistent nutrition guidelines for Australian ECEC services is a realistic recommendation, requiring relatively little modification.
This cross-sectional survey of long day care centres suggests that government-funded nutrition support for ECEC services is linked to improved knowledge, confidence and skills in planning healthy menus. While using these services may improve menu quality, it does not necessarily translate into compliance with the Victorian ECEC menu planning guidelines. Further research is needed to explore the benefits of assessing specific components of compliance (quality, quantity, variety), and to inform the development of more tailored support strategies.
Online surveys, on-site visits, and semi-structured interviews were conducted with ECEC services across Victoria, Australia, to assess breakfast provision against best practice guidelines. Only 10–16% of services met best practice criteria, and these were mostly located in socioeconomically advantaged areas. Key enablers included government funding and the use of nutrition guidelines. Barriers included time and budget constraints, staff shortages, and low confidence in applying nutrition guidance. Clear, practical breakfast guidelines are needed to improve breakfast quality in ECEC settings.
Nutrition environments in early childhood education: do they align with best practice?
This study assessed the content (comprehensiveness) and strength of written language in 118 publicly available ECEC centre-based nutrition policies (CBNPs) in Victoria, Australia, using the WellCCAT tool. Overall, policies had low median comprehensiveness (60/100) and very low median strength scores (17/100), which may be due to poor implementation of best practice in food provision and feeding practices.
This systematic review examined 82 studies to identify and evaluate tools used to measure food provision in ECEC and primary schools. Seven tools were identified, with the weighed food protocol being the most used and accurate for assessing individual intake. There is a need for a validated tool to assess food provision at the service level to better guide policy and practice.
This study validated a self-administered weighed food protocol (NUTRI_WASTE_ECEC) for measuring food provision and waste in ECEC settings. The protocol produced results equivalent to those collected by trained researchers, supporting its accuracy and potential for broader application. It offers a low-cost, scalable tool that ECEC services could use to monitor and improve menu quality, reduce food waste, and better understand children’s food preferences. Future research should assess the tool’s practicality and usability in real-world settings.
Playgroups
The Healthy Conversations @ Playgroup trial is a national randomised controlled study testing a peer-led program to support healthier eating, physical activity, screen time, and sleep habits in young children. Delivered through existing community playgroups, the low-cost, scalable program aims to equip parents with practical skills to prevent early childhood obesity. If proven effective, it offers a ready-to-implement solution with potential for broad uptake across Australia.
A qualitative evaluation of the Healthy Conversations @ Playgroup trial found that parents, playgroup coordinators, and facilitators valued the program for validating parenting practices, fostering shared experiences, and providing valuable peer support.
Where to begin? What are some different approaches?
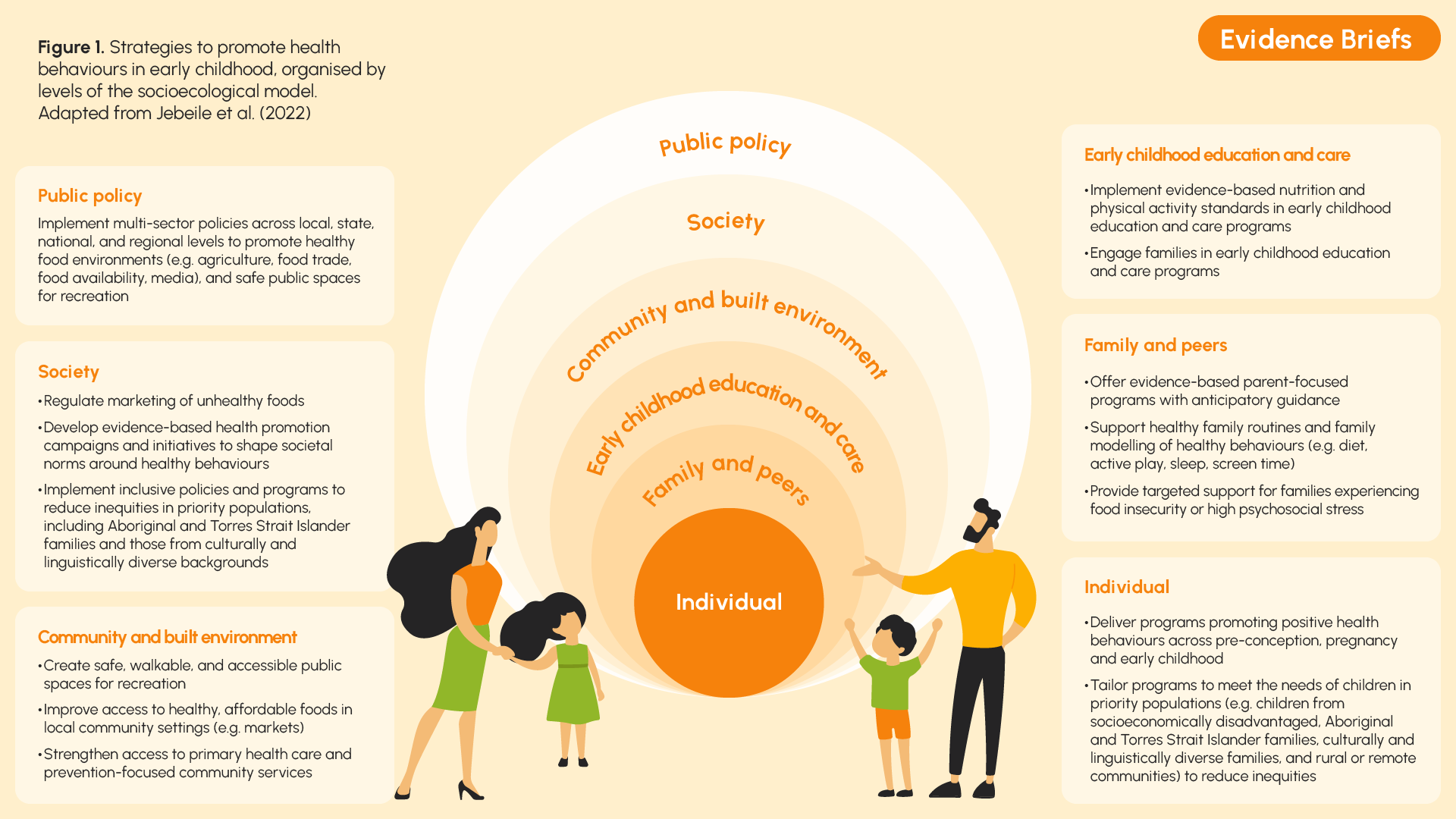
Obesity prevention in early childhood may focus on helping children and their families establish healthy eating and movement habits or on changing environments in which children live, grow and learn (Figure 1).
There are various evidence-based approaches to promote health behaviours developed in Australia and internationally.
Some focus on encouraging healthier behaviours (diet, physical activity, sedentary behaviour, sleep and screen time) in various settings such as home and early childhood education and care centres.
Others address the system drivers of obesity, including food labelling, marketing of discretionary foods, taxes and/or reformulation of sugary drinks, and access to green space and public transport.
Our research shows that individual programs alone are insufficient to reduce BMI at age 2. This may be due to the lack of system-wide actions across settings to address the multiple drivers of obesity. Early prevention should therefore be addressed as a broader suite of multi-level and multi-sectoral initiatives across the life course to promote healthy behaviours.
Evidence
Early life factors that affect obesity and the need for complex solutions
Obesity often begins in early childhood, a critical period that shapes future health. Our review of the evidence highlights the complex interplay of biological, sociocultural, environmental, and systemic factors influencing obesity development in early life. We emphasised the need for coordinated multi-level interventions and joined-up action across the first 2000 days to effectively address this multifaceted condition.
We outlined key opportunities to improve nutrition across the first 2000 days of life within national, state and local government systems, using policy, practice and research mechanisms. More joined-up action and greater program/policy coherence is needed, with funded capacity to facilitate the delivery of coordinated and integrated services to address nutrition in the first 2000 days.
We formed the TOPCHILD Collaboration, which brought together 31 randomised trials to create the largest early obesity prevention database to date of almost 30,000 children. We found that early family-based obesity prevention programs alone have no impact on children’s body mass index (BMI) by age two and most obesity-related health behaviours. This highlights the need for a broad and comprehensive range of actions across the life-course, systems and settings.
Intervention components for childhood obesity prevention
Health promotion for obesity prevention in children includes breastfeeding, healthy eating, active play, limiting screen time, and ensuring adequate sleep. Effective initiatives can be implemented at various levels, such as systems (e.g. policy, funding, partnerships, workforce training), settings (e.g. food environment, active play facilities), and individuals (e.g. programs and services). Initiatives that are embedded in the system are more likely to be sustained.
Policy makers should consider intervention components that are relevant to their contexts and environment, choosing those with a strong evidence base over those with less evidence. Ideally, program components need to be integrated into existing service delivery and should focus on reducing equity gaps.
Evidence
We looked at the various components of 37 different child obesity prevention initiatives from around the world within the TOPCHILD Collaboration. We found initiatives often aimed to support multiple child health behaviours, with the most common approach focused on all aspects of parental behaviours, including infant feeding, food provision and parent feeding, movement (active play/sedentary behaviour), and sleep health. The way these initiatives were delivered varied a lot. Most were led by a health professional, included training for facilitators, and included interactive parts with families. Initiatives also used lots of different strategies to support parent behaviour change. Unfortunately, despite the variation in approaches, none of these obesity prevention approaches appeared to reduce BMI at 2 years of age.
Digital or telephone-based support
AND
In this randomised clinical trial of Healthy Beginnings telephone or SMS support intervention, we found that telephone support increased rates of timely introduction of solid foods, early initiation of tummy time, and use of a cup. Both telephone and SMS support increased rates of having no screen time by 2 years of age and reduced bottle use at bedtime. Telephone support had greater effects than SMS in reducing screen time and improving eating behaviours. However, neither intervention had a significant effect on BMI.
We found that a staged telephone and SMS support intervention to mothers with children aged 2 years was associated with improved dietary and activity behaviours, but not BMI. The intervention was also associated with reduced children’s BMI at age 3 years only for those from lower income households.
The My Baby Now app offers credible, evidence-based breastfeeding support throughout the perinatal period and is highly regarded by users. First-time mothers valued its alignment with health professional advice and its development by credible experts. Mothers without university education rated the app to be higher quality, more useful and impactful than mothers with university education. This study highlights the potential of mHealth interventions to fill the gap in antenatal breastfeeding support, with users noting the lack of adequate information and guidance in routine prenatal care.
Tools
TOPCHILD-Policy Child Health Behaviour Evidence Dashboard – currently under development. Use the following link to express interest in participating in the dashboard user testing in 2025-26: https://researchsurvey.flinders.edu.au/surveys/?s=DCJ3EA7TW4DF3P8F
Evidence-based programs that can be scaled up
EPOCH-Translate has developed evidence for two programs that are available for scale up: Healthy Beginnings and INFANT. These programs target multiple health behaviours through anticipatory guidance and are delivered across multiple channels. While they showed improvements in health behaviours and support for parents, they had no impact on obesity outcomes, highlighting the need for additional complementary systemic changes to help address the multiple drivers of obesity.
Healthy Beginnings Home-based Program
Healthy Beginnings is a staged early intervention program to prevent childhood obesity, run in partnership with the University of Sydney and Local Health Districts in NSW.
It involves eight home visits by Child and Family Health Nurses from late pregnancy to age 2, focusing on improving family and behavioural risk factors for childhood obesity, such as improving infant feeding practices. For parent resources related to the Healthy Beginnings program, please see the Healthy Beginnings website.
Evidence
The Healthy Beginnings home-based program involved Child and Family Health Nurses delivering 8 home visits, starting in the third trimester and continuing with 7 additional visits at 1, 3, 5, 9, 12,18 and 24 months after birth. Most participants were from socially and economically disadvantaged areas of Sydney. In this randomised trial, we found significant improvements in duration of breastfeeding, appropriate timing of introduction of solids, and practice of “tummy time” and a reduction in mean BMI among those receiving the home-based intervention. There were no significant differences between the groups with regard to consumption of fruit, consumption of “junk food,” or time spent in outdoor play at 24 months.
Tummy time activities can strengthen infants’ neck and shoulder muscles and improve motor skills, which are crucial for more complicated movements, such as sitting, rolling over, crawling, and pulling bodies to a standing position, as well as enhanced motor development. The Healthy Beginnings intervention improved practice of tummy time including early start and daily practice of tummy time.
INFANT
The INFANT program, developed by Institute for Physical Activity and Nutrition and implemented in partnership with Victorian Department of Health and multiple other practice partners, provides anticipatory guidance on feeding, active play and screen time from birth to 18 months of age. It consists of four group sessions delivered by trained health and early years professionals and complemented by a mobile phone app for parents. For parent resources related to the INFANT program, please see the INFANT program website.
Evidence
A parent-focused intervention to reduce infant obesity risk behaviors: a randomized trial
This study evaluating the effectiveness of the INFANT program showed that participating in INFANT led to positive health outcomes for children at age 20 months, with reduced consumption of discretionary food and less television viewing. There was no effect on BMI z-scores.
We showed that the intervention effect from the INFANT program remained evident for reduced consumption of discretionary food at ages 3.5 and 5 years (2 and 3.5 years post-intervention). While the reduction in television viewing time remained consistent, it was no longer statistically significant. It also showed that additional benefits of the program became apparent longer term, with children whose families had participated in INFANT also having higher fruit, vegetable, and water intake and lower consumption of discretionary drinks. There remained no evidence for effect on zBMI, waist circumference z-score or physical activity.
Quantifying the overall impact of an early childhood multi-behavioural lifestyle intervention
We reported on the effectiveness of INFANT in changing children lifestyle patterns showing the program was effective in improving unhealthy lifestyle patterns incorporating behaviours including consumption of discretionary food and drinks and TV viewing.